2019-20 Pre-Budget Submission
Date: 1 February 2019
Priorities for the 2019-20 Federal Budget
More affordable medicines
Prime Minister Scott Morrison:
“In healthcare, I am distressed by the challenge of chronic illness in this country and those who suffer from it. Affordable medicines, aged care, Medicare, small and medium sized businesses, and to ensure that we are continuing to deliver the encouragement and support to that enterprise ethic that exists across our economy. There are some key early priorities”.
24 August 2018
Introduction
The Pharmacy Guild of Australia (‘the Guild) welcomes the opportunity to provide a pre-Budget submission to the Coalition Government for the 2019‑20 Federal Budget.
The Guild congratulates the Federal Government for funding new listings of medicines on the Pharmaceutical Benefits Scheme (PBS), some of which are lifesaving medicines previously unaffordable to patients.
While new listings on the PBS enhance the affordability of these medicines, the broader population experiences official PBS co-payment rises each year, including concessional patients. PBS pricing policies, including price disclosure, continue to reduce the amount paid by government for many PBS medicines benefiting general patients when they have under co-payment scripts filled, but concessional patients receive little or no direct financial benefit from these policies. Since January 2016, pharmacists have had the option to discount the PBS patient co-payment for claimable PBS prescriptions by up to $1. This has proven to be an ineffective way to provide more affordable access to PBS medicines, and has instead increased inequity and undermined the universality of the PBS while commoditising medicine usage.
Medicine costs are a highly visible out-of-pocket cost, which become more pronounced as Australians age and are likely to become more reliant on medicines. There are 185 million PBS subsidised prescriptions dispensed to concessional patients annually, so the affordability of medicines is of paramount importance to many Australians.
2019-20 Budget priority: The Guild recommends that the 2019-20 Federal Budget improves medicines affordability by removing the optional $1 discount and reducing the PBS and RPBS co-payments by $1 for all patients. |
Background
As a result of Federal Government policy through the 6th Community Pharmacy Agreement (6CPA) budget savings measures, from 1 January 2016, pharmacists have been able to discount the PBS patient co-payment by up to $1. The Guild did not support this measure at the time of the 6CPA because it undermines universality of the PBS.
On one hand, the intention of the Government policy is to make medicines cheaper for patients through promoting competition between pharmacies. On the other hand, the amount the patient pays determines when annual safety-net thresholds are reached (after which PBS medicines are free for concessional patients and further subsidised for general patients).This means that accessing the $1 discount results in patients taking longer to reach their safety-net threshold. For the Australians who are the most reliant on PBS medicines, particularly those individuals and families with multiple chronic conditions, PBS medicines are no more affordable over a 12 month period than they were before the discount was introduced. The policy creates budget savings for the Federal Government from not having to pay the higher PBS subsidies when patients reach the safety network from as early in the year as they otherwise would.
At the time of announcing the policy, the Federal Government estimated the $1 discount policy would result in Federal budget savings of $373.4 million over 4.5 years. The much lower than anticipated take-up of the optional $1 discount means these savings are not being realised, with only 28 per cent of eligible prescriptions discounted.
The reality and the rationale for abolishing the $1 discount
Despite the intention of making medicines cheaper for patients and reaping budget savings from patients taking longer to reach their safety net thresholds, the reality has been much different.
Updated PBS data published by the Department of Health in January 2019 for the 2017‑18 financial year (reproduced as Table 1 below) shows that only 28 per cent of eligible prescriptions have been discounted. This is consistent between general and concessional PBS patients, and patients under the Repatriation Schedule of Pharmaceutical Benefits (RPBS) fare even worse with only 17 per cent of eligible prescriptions discounted.
Table 1: Subsidised PBS/RPBS prescriptions dispensed by community pharmacies
2017-18 | Concessional | General | RPBS | Total | ||||
Prescription type | Prescriptions | % | Prescriptions | % | Prescriptions | % | Prescriptions | % |
Discounted | 52,201,149 | 28 | 4,452,294 | 28 | 1,501,647 | 17 | 58,155,090 | 28 |
Non-discounted | 131,908,236 | 72 | 11,725,425 | 72 | 7,290,844 | 83 | 150,924,505 | 72 |
Total | 184,109,385 | 100 | 16,177,719 | 100 | 8,792,491 | 100 | 209,079,595 | 100 |
Source: Department of Health, Expenditure and Prescriptions Twelve Months to 30 June 2018, available at: https://www.pbs.gov.au/info/statistics/expenditure-prescriptions/pbs-expenditure-and-prescriptions
Clearly, the $1 discount policy has not resulted in an aggregate take-up that has meaningfully contributed to lower medicine prices for the broader population.
Universality of the PBS
The $1 discount policy has not only failed to result in an aggregate take-up that has meaningfully contributed to lower medicine prices; it has created unfair geographical divergences in the prices that patients with the same health conditions pay for the same subsidised PBS medicines – undermining the universality of the PBS and arbitrarily creating different classes of patients. This is evident from Chart 1 sourced from the independent Review of Pharmacy Remuneration and Regulation (‘the Review’) interim report in June 2017.
Chart 1: prevalence of $1 discount across PhARIA (6 months to July 2016)
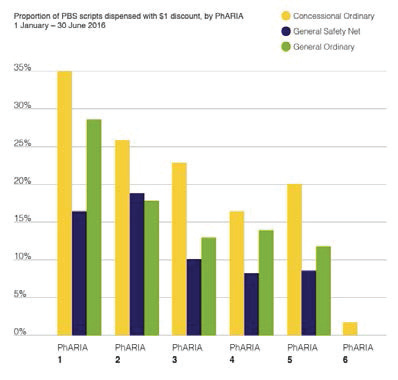
Source: Review of Pharmacy Remuneration and Regulation – Interim Report – June 2017, Available at: http://www.health.gov.au/internet/main/publishing.nsf/content/review-pharmacy-remuneration-regulation
The chart shows that the prevalence of discounting varies significantly by Pharmacy Access/Remoteness Index of Australia (PhARIA) geographic region where PhARIA 1 represents urbanised regions and PhARIA 6 remote regions.[1]
People in rural and remote areas are likely to pay more for medicines under the optional $1 co-payment discount policy than their counterparts in metropolitan areas. Moreover, general patients in a big capital city who are more likely to be able to afford medicines receive more discounts than concessional patients with a chronic condition in a regional area. Why should this be the case? How is this good policy?
The failure of the $1 discount policy in terms of universality and patient health outcomes was specifically highlighted by the Government’s Pharmacy Remuneration and Regulation Review. For example, the Review’s Final Report concludes:
“The $1 discount has not led to equitable outcomes for consumers” [2],
and its associated recommendation:
“The Australian Government should abolish the $1 discount on the PBS patient co-payment”.
The Review’s Final Report further effectively suggests that using the $1 discount is not the right tool to promote lower medicine costs for patients and instead states:
“…if the government considers that lower co-payments are desirable, they should lower them for all consumers,…”
The implication of the above statement is that the Federal Government could directly reduce patient out-of-pocket medicine costs by cutting official PBS co-payments. As an example, Chart 2 below shows the historical growth in the co-payment for concessional patients and how a $1 co-payment reduction would result in an immediate and universal 15% reduction in the cost of concessional prescriptions for approximately 1 million concessional patients – the same patients who have received little or no direct benefit from over 10 years of PBS pricing policies that have produced very large budget savings for government.
Chart 2: Concessional patient co-payment growth ($)
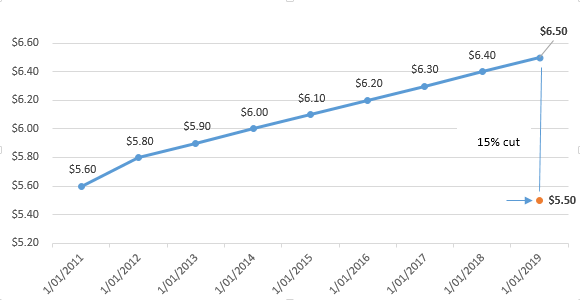
Source: PBS website and historical reports.
Reducing patients’ out-of-pocket costs will make it easier for Australians, particularly pensioners and low-income earners, to afford the medicines they are prescribed, leading to better Quality Use of Medicines, improved overall health outcomes and reduced incentive to ration.
The net budgetary cost of the removal of the optional $1 co-payment discount and introducing a $1 reduction to PBS co-payments from 1 January 2020 is estimated to be around $500 million over four years. When considered in the context of promoting quality use of medicines, the Review noted:
“Consistency in the price that consumers pay for their PBS-listed medicines could improve health outcomes,…”.
The funding of more affordable medicines would be a prudent investment by the Federal Government in better health outcomes. Moreover it is affordable given the ongoing budget savings from the medicine supply chain in Australia (see Budget savings section below).
Evidence of unaffordable medicines
Medicine affordability is an ongoing issue and there is clear evidence that a significant proportion of Australians have difficulties affording to have their prescriptions filled as a result of higher out-of-pocket medicine costs.
Household expenditure data for Australia shows that medicines and pharmaceutical products account for 26% of total weekly spending on health for the lowest income households, compared to 18% for all households.[3] Research for Australia highlights the widespread sensitivity of patients’ medicine use to cost - the 21% increase in patient co‑payments in 2005 adversely affected prescription medicine use in all areas of Australia, not only remote or disadvantaged areas.[4]
The percentage of adults who have avoided filling a prescription due to cost in the preceding 12 months is persistently above 7% even as general patients have had their out-of-pocket costs reduced for under co-payment scripts as PBS medicine prices have been reduced through price disclosure. One in eight Australians with fair or poor health delayed getting or did not get prescribed medication due to cost in 2016‑17.[5]
Around 87% of people aged 65 and over had at least one chronic disease in 2014-15.[6] Research has shown that the financial burden associated with medicines used for the management of chronic conditions by Australian patients is substantial and is compounded by the ongoing need for multiple medicines.[7] Moreover, there is a body of clear evidence demonstrating that medication non‑adherence places a significant cost burden on healthcare systems, increasing overall government expenditure on health.[8]
Increases in patient co-payments make medicines less affordable with delays in filling and non-filling of prescriptions increasing costs across the broader health systems. This runs counter to the Morrison Government’s important policy priority of affordable PBS medicines for all Australians.
Competition
One intention of the Government’s $1 discount policy is to make medicines cheaper for patients through promoting competition between pharmacies. There are a number of problems with respect to the efficacy of the $1 discount policy as a means of promoting competition and in turn lowering prices that enhance patient welfare.
Foremost, competition itself should not be the primary or end goal for PBS medicines as patients’ welfare depends on more fundamental aspects than price competition. Medicines are not normal products of commerce – specifically prescription medicine is not the same as a consumer picking an item off the supermarket shelf based on their preferences and price comparisons. Prescription medicines require clinical expertise, care and advice from a trained pharmacist. This has been pointed out by the Review’s Final Report:
“The removal of pricing discretion may appear to be inconsistent with standard retail competition. Yet PBS medicines are not provided through standard retail mechanisms. A consumer cannot simply demand a PBS-listed medicine. Consumers can only access such medicines when an approved medical practitioner has determined that they are required to treat a medical condition”.
This quote is from a Review headed up by Professor Stephen King, a recognised competition policy economist, who you would expect would take the ‘competition is good’ line but in this case does not. Instead, the Review states:
“The Panel considers that, when pharmacies compete for a consumer’s business, it should be on the quality of the service that is provided to the consumer as opposed to PBS medicine prices”.
Hence the quality of that care and service is much more important to the patient’s welfare than haggling over a $1 discount. Quality use of medicines is ultimately what medicine should be about instead of price competition.
Even if the argument is that price competition is important to patients’ welfare - the $1 discount policy has done little to contribute to widespread competition. As noted earlier, only 28 per cent of prescriptions have been discounted. Effectively, all the $1 discount policy has done is entrench competition where it was already strong – in localised highly urban areas where competition is already strong in relation to non subsidised medicines below the patient co-payment as well as for non-prescription medicines and other pharmacy products. As a result, it has helped create an environment where discounting of PBS medicines is used by some in the sector as a means of enticing customers for ancillary products such as cosmetics and complementary medicines.
Does the Government really want PBS medicines to be used as a retail marketing tool to sell non-health products in pharmacies? Where the Quality Use of Medicines is promoted in such a business model is unclear. Quoting the Review again:
“…where competition is strong, pharmacies will use the discretion given by the $1 discount as part of their competitive strategy, albeit possibly reducing competition on other dimensions such as service”.
Equity is another issue with the failed $1 discount policy. As noted earlier, discounting has been sporadic geographically with rural patients and RPBS patients largely missing out. Surely this is not the Government’s intended outcome - for rural patients to be second rate patients who do not share the advantages of urban based patients? The Review Final Report states:
“Having varying levels of competition in community pharmacy in different parts of Australia creates issues of equity for consumers. The $1 discount simply highlights and possibly exacerbates these inequities. It does not address them”.
Commoditising medicines and dispensing
The $1 discount policy has failed as a policy by creating an environment that commoditises medicine as another ‘consumable’ where patient and pharmacist negotiate on price rather than focusing on the health outcome aspects of dispensing. To quote the Review again:
“PBS medicines are not normal items of commerce”.
Pharmacists should be able to focus their time on providing professional care and advice to patients about their medicines, competing as health professionals based on the quality of service and care, rather than having conversations focused on whether a patient can get a dollar off or not.
The optional $1 co-payment discount has commoditised and devalued the importance of safe dispensing of PBS medicines and, in doing so, reduced the emphasis on the quality use of government-subsidised medicines and the core objectives of the National Medicines Policy.
Budget savings
The failure of the $1 discount policy as a means of creating budget savings through the PBS is also evident in the Government’s own figures. As mentioned earlier, the original estimate was that, from January 2016, the Federal Government would reap budget savings of $373.4 million over 4.5 years. The reality is nowhere near this estimate, with internal Guild modelling suggesting over the same 4.5 year period that the estimated savings will be around $108 million, barely a third of the intended budget savings. Recent work with the Department of Health indicates that the minimal budget savings expected from the $1 discount policy will continue beyond 2020.
Hence, any foregone budget savings as a result of abolishing the $1 discount policy are minimal and have no material bearing on the fiscal sustainability of the PBS and broader Federal Budget. Moreover, any foregone budget savings are dwarfed by the very large, ongoing estimated budget savings from price disclosure (Chart 3) that have ensured that the PBS is arguably the most fiscally controlled part of the health budget.
Chart 3: Estimated savings to Federal Budget from price disclosure ($ billion)
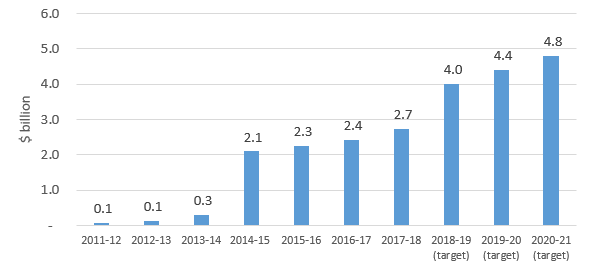
Source: successive Budget Papers and Department of Health Annual Reports.
The Guild’s efforts to address this issue
The Guild has been seeking Federal Government support for the Review’s recommendation that the $1 discount be abolished. The Federal Government’s response to the Review in May 2018 stated that:
“The Government has previously agreed, as part of its May 2017 Compact with the Guild, to review the $1 discount on the PBS patient co-payment (the $1 Discount Review) following the report of the Review of Pharmacy Remuneration and Regulation. The Government will further consider this recommendation once the $1 Discount Review has been completed”.[9]
The Guild is aware from communications with the Department of Health that the $1 Discount Review has been underway for a number of months and the 2019‑20 Budget provides the opportunity to discontinue this flawed and failed policy.
Conclusion
More affordable medicines can be immediately achieved by removing the discretionary $1 discount and reducing official patient co-payments by $1. Abolishing the optional $1 discount and reducing co-payments will mean that all Australians will have more affordable, equitable and universal access to the PBS, regardless of where they live or which pharmacy they choose and whether they are concessional or general patients. Rural and remote patients will have equally affordable access to the PBS as patients in capital cities, and community pharmacists everywhere will be able to focus entirely on providing the best medicine related care and advice, rather than having conversations with patients about whether they can get a dollar off or not.
The Pharmacy Guild of Australia calls on the Federal Government, through the 2019-20 Budget, to:
|
About the Pharmacy Guild of Australia
The Guild is a national employers’ organisation with over 90 years of experience in representing and promoting the value of the role of community pharmacy in the Australian health care system. Community pharmacies are a vital part of our national health system with the potential to make an even bigger contribution to the health of all Australians.
The Guild shares with the Federal Government responsibility for the implementation of the National Medicines Policy, as evidenced by successive Community Pharmacy Agreements (CPA) enshrined in the National Health Act 1953, including the current 6th CPA underpinned by the shared principles of:
- Stewardship of the health system and a shared responsibility for the stewardship of the PBS.
- Partnership in the implementation of Australia’s National Medicines Policy.
- Stability and certainty of the Government’s investment in the medicine supply chain, as well as timely availability of medicines through a well-distributed community pharmacy network.
- Integrity of Australia’s health system, including patient safety and high value clinical care.
The Guild and the broader community pharmacy network have made significant contributions to the achievement of the National Medicines Policy objectives for patient outcomes, while at the same time enabling the ongoing (fiscal) stability of the PBS by working with successive Governments on budget savings measures.
Download the full submission here.
Contact: Sanja Pavlak
Page last updated on: 22 April 2020